The Common Vein Copyright 2010
Introduction
The term prostate is derived from Greek- prostates, which means “one who stands before”, “protector”, “guardian” owing to its position relative to the bladder although it appears that Herophilus who named the organ implied that it lay before the testes.
It is cradled by the urinary bladder, and fits snugly between the bladder and the membranous and penile urethra. It provides passage both for urine, and semen but also acts as the mixing pot for semen where the ingredients come together.
The prostate sits between the internal and external sphincters that control the urinary stream. At the bladder neck the detrusor muscle of the bladder becomes confluent with the internal sphincter while smooth muscle of the anterior fibromuscular zone contributes to the internal sphincter as well. On the inferior side, the external urethral sphincter is formed from skeletal muscle from the inferior aspect of the fibromuscular layer and the participation of the perineal membrane. The external sphincter surrounds the membranous urethra and the beginning of the penile urethra. Thus it is interesting as well that the anterior zone of the prostate contains smooth muscle superiorly and skeletal muscle inferiorly. It shares this unique characteristic of having both smooth muscle and skeletal muscle with the esophagus.
|
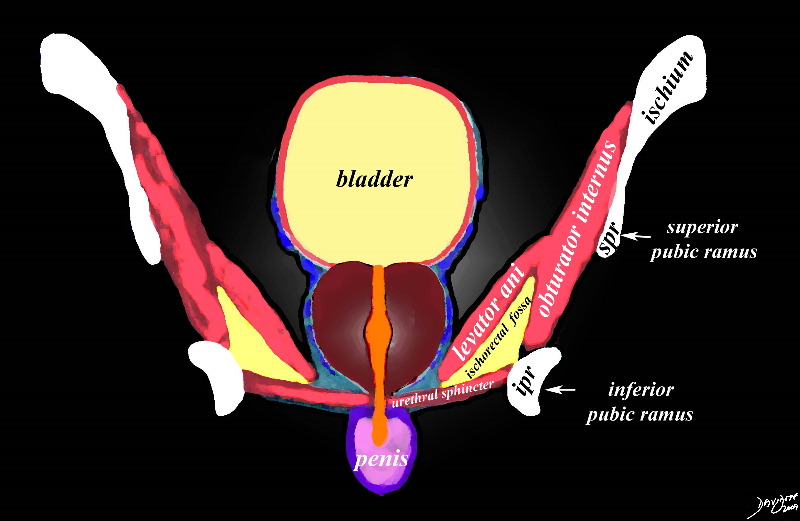
The Prostate in Context Coronal Projection |
|
The diagram reflects the position of the prostate (maroon overlay) and surrounding structures as seen in the coronal plane. The bladder lies superiorly and rests on the base of the prostate (maroon), which in turn has its apex resting on the pelvic floor. The prostatic urethra (orange) traverses the middle of the prostate. The prostate is immediately surrounded by the capsule and periprostatic venous plexus (blue tubular structures). The levator ani and obturator internus muscles with the ischiorectal fossa and components of the ischium and pubic bones form the inferolateral border on either side. The urethral sphincter acts as the inferior border, below which is the membranous urethra, the base of the penis and penile urethra. Image Courtesy Ashley Davidoff Copyright 2010 99651b16.8s |
Sagittal Projection
The anterior and posterior relationships of the prostate are appreciated in this projection.. The prostate lies immediately behind the pubic symphisis. Between the prostate and the pubic symphisis is the retropubic space of Retzius in which the anterior venous plexus of Santorini is positioned
Posteriorly, the Denonvilliers’ fascia is found and is made up of a combination of posterior prostatic and anterior rectal coverings. As we have noted in the coronal projection the prostate sits on the perineal membrane. The urethra runs through it, and extends through the membrane, after which it changes direction to enter the shaft of the penis. This change in direction of the urethra is best appreciated in the sagittal projection. Posterolaterally, the prostate is cradled between the levator ani muscles.
|
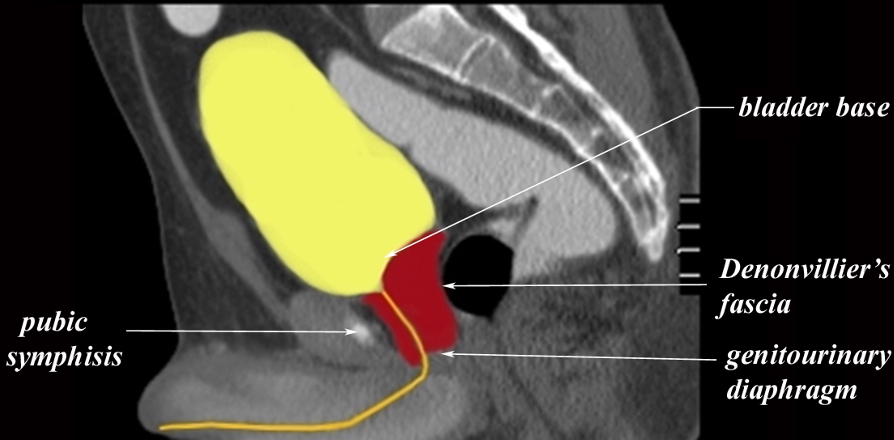
Immediate Neighbors of the Prostate |
|
The CTscan reflects a normal prostate seen in the sagittal plane. The bladder is distended. Note the position of the prostate posterior to the pubic symphisis and anterior to the rectum (black bubble) covered posteriorly by Denonvillier’s fascia. Superiorly it supports the bladder base and inferiorly it is supported by the perineal membrane. (genitourinary diaphragm) The bladder is overlaid in yellow and the urethra is the channel overlaid in orange. Image Courtesy Ashley Davidoff Copyright 2010 99331c02g03.9 |
Applied Biology
The ideal route for examining the prostate is via the rectum, whether one is performing a digital examination or imaging with ultrasound or MRI, due to the proximity of the two organs.
The relationship to the prostate and the urethra is also intimate. When the transitional zone of the prostate enlarges due to hyperplasia it obstructs the urethra resulting in partial obstruction clinically manifesting in a progressively reduced force of the urinary stream. Post void residual increases and the patient then needs to void more frequently. In addition during micturition the bladder muscle tires as it tries to expel the full volume of urine but recovers a short time thereafter (a few seconds) and the patient usually will void an additional small volume after the short rest period. This clinical syndrome resulting from bladder obstruction is called prostatism or more recently referred to as LUTS – lower urinary tract symptoms.